
Omega-3 fatty acids for dogs: how EPA and DHA support cartilage, joint comfort, cardiovascular function, brain health, and skin, with a clinical framework for individualized dosing using the Omega-3 Index and iFATS score.
Key Takeaways: Omega-3 Fatty Acids for Dogs
- EPA and DHA are essential for dogs — dogs cannot synthesize them in clinically meaningful amounts and must obtain them from marine sources, since dogs convert plant-based ALA to EPA/DHA at single-digit efficiency.
- Joint comfort is the most evidence-supported indication — multiple randomized controlled trials, including Mehler et al. (2016), have demonstrated measurable clinical and biomarker improvement in dogs with osteoarthritis.
- Dose by combined EPA + DHA, not total fish oil — clinical targets range from 200–500 mg/day for small dogs to 2,200–3,500 mg/day for giant dogs, divided with meals.
- Allow 8–12 weeks for full clinical effect — cell membrane fatty acid composition turns over gradually; expect onset over weeks, not days.
- Quality matters as much as dose — natural triglyceride form, low oxidation status, and verified EPA + DHA content per serving determine real-world clinical response.
Nutraceutical Interventions
Few nutraceutical interventions in canine medicine carry the depth of peer-reviewed evidence that Omega-3 fatty acids for dogs — specifically the long-chain marine omega-3 fatty acids EPA (eicosapentaenoic acid) and DHA (docosahexaenoic acid) — has accumulated over the past two decades. Specifically, multiple randomized controlled trials have now demonstrated meaningful clinical benefit of EPA and DHA supplementation in dogs with osteoarthritis, with parallel mechanistic and observational support across cardiovascular, neurological, dermatologic, renal, and ocular systems.
This guide is written for both veterinarians and the dog owners they advise. In particular, it covers the biology of EPA and DHA, the multi-organ system benefits across canine physiology with particular emphasis on cartilage and joint health, the most clinically important randomized controlled trial in the canine literature, why individual variability in omega-3 processing matters, and how the iFATS (Inflammatory Fatty Acid Test Score) and Omega-3 Index can be used to individualize and verify therapy.
All content reflects the same evidence standards I’ve applied throughout my academic career and three decades of clinical practice in veterinary anesthesia and pain management.
In This Article
- Why Omega-3 Fatty Acids for Dogs Matters: The Essential-Fatty-Acid Argument
- EPA, DHA, and ALA: What Each Omega-3 Does in the Canine Body
- Mechanism of Action: How Omega-3 Fatty Acids Modulate Inflammation in Dogs
- Omega-3 Fatty Acids and Canine Joint Health: Cartilage, Synovium & the Inflammatory Cascade
- Featured Research: Mehler et al. (2016) — The Definitive RCT on EPA/DHA in Canine Osteoarthritis
- Multi-Organ System Benefits: Heart, Brain, Skin, Kidneys & Eyes
- Individual Variability: Why Two Dogs on the Same Dose Get Different Results
- The Omega-3 Index and iFATS: Personalizing Omega-3 Fatty Acids for Dogs
- Omega-3 Dosage for Dogs: EPA + DHA Targets by Body Weight & Indication
- Quality Matters: Triglyceride Form, Oxidation & Third-Party Testing
- Integrating Omega-3 Fatty Acids for Dogs into a Multimodal Joint Wellness Protocol
- Peak Therapeutics Canine Omega Benefits: Formulation & Quality Standards
- Frequently Asked Questions — Omega-3 Fatty Acids for Dogs
- References
- About Dr. James S. Gaynor, DVM, MS, DACVAA
1. Why Omega-3 Fatty Acids for Dogs Matters: The Essential-Fatty-Acid Argument
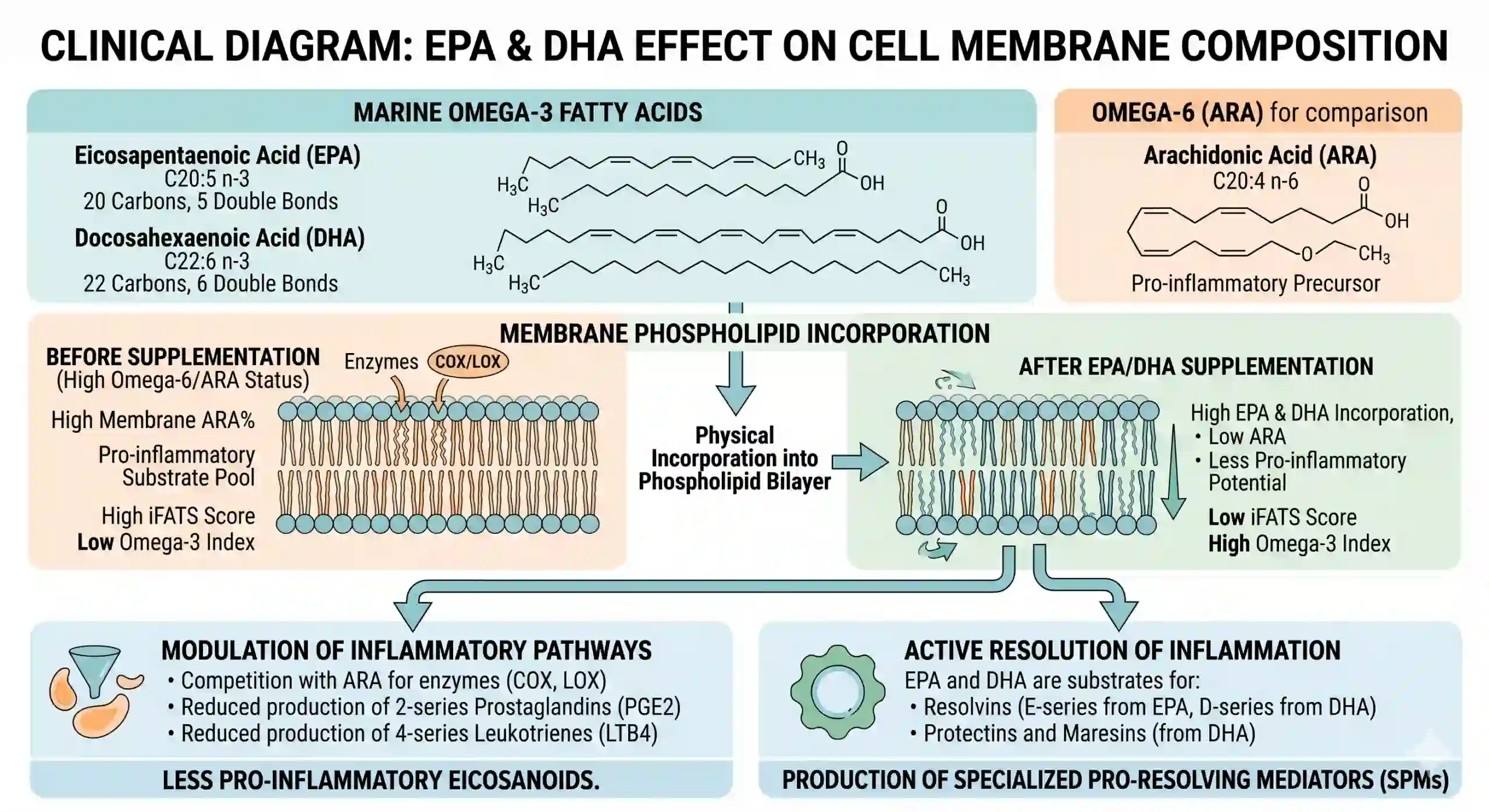
Omega-3 fatty acids are classified as essential because dogs cannot synthesize them in physiologically meaningful amounts. Therefore, they must be obtained through the diet, and in modern commercial dog food, the omega-6 to omega-3 ratio is typically skewed heavily toward omega-6 due to the prevalence of corn-fed animal products and refined seed oils.
This dietary ratio matters because omega-6 fatty acids (particularly arachidonic acid, ARA) are the precursors to pro-inflammatory eicosanoids, while omega-3 fatty acids — EPA and DHA — are the precursors to specialized pro-resolving mediators (resolvins, protectins, and maresins) that actively resolve inflammation.
Implications
The clinical implication is direct: most dogs on commercial diets are operating in a pro-inflammatory fatty acid environment at the cell membrane level. However, supplementation with EPA and DHA from a quality marine source measurably shifts this balance, with downstream effects across every organ system that depends on healthy inflammatory signaling, which is to say, every organ system.
In short, this is the biological foundation underlying the broad evidence base for marine EPA and DHA supplementation across joint, cardiovascular, neurological, renal, dermatologic, and ocular indications.
2. EPA, DHA, and ALA: What Each Omega-3 Does in the Canine Body
Not all omega-3 fatty acids are clinically equivalent. For this reason, veterinarians and dog owners evaluating omega-3 products should understand the practical differences between the three principal omega-3 species:
Omega-3 Fatty Acid |
Function & Clinical Relevance in Dogs |
|---|---|
| EPA (Eicosapentaenoic Acid) | The primary anti-inflammatory omega-3. EPA competes with arachidonic acid (ARA) at the cyclooxygenase and lipoxygenase enzymes, producing less inflammatory eicosanoids and serving as the precursor to E-series resolvins. Notably, EPA is the most clinically relevant omega-3 fatty acid for canine joint comfort, cardiovascular support, and inflammatory dermatologic conditions. Marine-sourced. |
| DHA (Docosahexaenoic Acid) | The structural omega-3. DHA is incorporated into neuronal membranes, retinal photoreceptors, and cardiac tissue, where it supports membrane fluidity and signal transduction. Additionally, DHA is the precursor to D-series resolvins, protectins, and maresins. Critical for puppy neurological and visual development, cognitive function in seniors, and a meaningful contributor to anti-inflammatory activity in adult dogs. Marine-sourced. |
| ALA (Alpha-Linolenic Acid) | The plant-derived omega-3 (flaxseed, chia, hemp). ALA must be enzymatically converted to EPA and DHA to exert biological activity, and dogs convert ALA to EPA and DHA very inefficiently, with single-digit conversion rates reported. Consequently, plant-based omega-3 sources alone are inadequate to achieve clinically meaningful EPA and DHA levels in dogs. Marine sources are required for clinical dosing. |
| ARA (Arachidonic Acid) | Not an omega-3; included here for context. ARA is the dominant omega-6 fatty acid in cell membranes and the precursor to pro-inflammatory prostaglandins, thromboxanes, and leukotrienes. Specifically, the ratio of ARA to (EPA + DHA) at the cell membrane level is the central inflammatory marker measured by the iFATS score (see Section 8). |
3. Mechanism of Action: How Omega-3 Fatty Acids Modulate Inflammation in Dogs
EPA and DHA exert their clinical effects through several converging biochemical mechanisms. In particular, understanding these is foundational to understanding why marine omega-3 supplementation has demonstrable, mechanism-based benefit across multiple organ systems, not merely the systemic effect of a generic anti-inflammatory.
Mechanism |
Clinical
Relevance in Dogs |
|---|---|
| Membrane phospholipid incorporation | EPA and DHA are physically incorporated into the phospholipid bilayer of every cell, partially displacing arachidonic acid. As a result, this shifts the substrate pool for inflammatory enzymes and produces measurable changes in cell membrane fatty acid composition, the basis for the Omega-3 Index and iFATS score (Section 8). |
| Reduced pro-inflammatory eicosanoids | With less ARA in the membrane, COX and LOX enzymes produce fewer 2-series prostaglandins (PGE2), 2-series thromboxanes, and 4-series leukotrienes (LTB4), the pro-inflammatory mediators driving joint pain, vascular inflammation, and tissue damage. |
| Production of specialized pro-resolving mediators (SPMs) | EPA and DHA serve as substrates for resolvins, protectins, and maresins, endogenous mediators that actively resolve inflammation rather than merely suppress it. Importantly, this distinguishes omega-3s from NSAIDs, which block enzymes but do not promote resolution. |
| NF-κB signaling modulation | EPA and DHA modulate NF-κB activation, reducing transcription of pro-inflammatory cytokines including TNF-α, IL-1β, and IL-6, central drivers of cartilage matrix degradation in canine osteoarthritis. |
| Cartilage matrix preservation | EPA reduces cartilage explant expression of aggrecanases (ADAMTS-4, ADAMTS-5) and matrix metalloproteinases (MMPs), the enzymes responsible for proteoglycan and collagen degradation in osteoarthritic cartilage. Notably, this is a structural mechanism, not just a symptomatic one. |
4. Omega-3 Fatty Acids and Canine Joint Health: Cartilage, Synovium & the Inflammatory Cascade
The Scale of Canine Osteoarthritis
Joint comfort and mobility is the single most evidence-supported indication for Omega-3 fatty acids for dogs, and the area where I most consistently incorporate EPA and DHA into multimodal pain management protocols. Canine osteoarthritis (OA) affects a substantial proportion of adult and senior dogs.
In fact, estimates from imaging studies suggest that the majority of dogs over the age of 8 have radiographic evidence of OA, even when clinical signs are subtle.
The pathology of canine OA involves progressive cartilage matrix degradation, low-grade synovitis, subchondral bone remodeling, and peripheral and central nociceptive sensitization. EPA and DHA address multiple nodes in this cascade simultaneously, which is why omega-3 supplementation has been shown to produce measurable benefit in randomized controlled trials, including improved owner-assessed quality of life, improved veterinarian-assessed lameness scores, and in some studies, reduced concurrent NSAID requirement.
Tissue-Level Effects Across the Joint
Joint-Tissue Compartment |
Effect of EPA & DHA |
|---|---|
| Articular cartilage | EPA reduces chondrocyte expression of aggrecanases and MMPs, slowing proteoglycan and collagen degradation. Additionally, it reduces IL-1β-driven catabolic signaling in chondrocyte cultures. The cartilage-protective mechanism is structural, not solely symptomatic. |
| Synovial membrane | Reduces synovial macrophage activation and pro-inflammatory cytokine release. Lower synovitis = lower joint effusion, less pain on flexion, improved range of motion. This is particularly relevant in the early-to-moderate OA window where synovitis is a major pain driver. |
| Subchondral bone | Modulates osteoclast/osteoblast balance via reduced PGE2 signaling. Furthermore, it may limit subchondral bone remodeling that contributes to chronic OA pain in advanced disease. |
| Peripheral nociceptors | Reduced local PGE2 and LTB4 reduce peripheral nociceptor sensitization. Clinically: less pain on weight-bearing, less pain after activity, reduced morning stiffness reported by owners. |
| Cartilage repair signaling | Resolvins and maresins derived from EPA/DHA support tissue repair signaling pathways. Active resolution of inflammation, not merely suppression. |
Clinical Timeline for Joint-Comfort Response
In clinical practice, the joint-comfort benefit of EPA and DHA supplementation typically becomes apparent at 8–12 weeks of consistent daily supplementation, meaningfully slower than NSAID onset, but with a fundamentally different mechanism and risk profile. This time course reflects the underlying biology: cell membrane fatty acid composition turns over gradually, and the iFATS shift driving clinical benefit is a multi-week process. For this reason, owners should be counseled to expect onset over weeks rather than days.
5. Featured Research
Mehler et al. (2016) — The Definitive Randomized Controlled Trial on EPA/DHA in Canine Osteoarthritis
Among the multiple randomized controlled trials of omega-3 fatty acids in canine osteoarthritis, the Mehler et al. (2016) study warrants particular attention, both because of its rigorous design and because it explicitly correlated red blood cell membrane fatty acid changes with clinical outcomes, providing a mechanistic and biomarker-based bridge between dose, biology, and measurable benefit.
Featured Research: EPA, DHA & Canine Osteoarthritis
Study: Mehler SJ, May LR, King C, Harris WS, Shah Z. A prospective, randomized, double-blind, placebo-controlled evaluation of the effects of eicosapentaenoic acid and docosahexaenoic acid on the clinical signs and erythrocyte membrane polyunsaturated fatty acid concentrations in dogs with osteoarthritis. Prostaglandins, Leukotrienes and Essential Fatty Acids. 2016;109:1–7. doi:10.1016/j.plefa.2016.03.015
Design: Prospective, randomized, double-blind, placebo-controlled clinical trial in 78 client-owned dogs with confirmed osteoarthritis. Dogs received either an EPA/DHA fish oil supplement or placebo daily, with assessment of clinical signs and red blood cell membrane fatty acid composition over the study period.
Primary biomarker — iFATS: The investigators evaluated the iFATS™ (Inflammatory Fatty Acid Test Score), a novel algorithm based on the membrane ratio of arachidonic acid to (EPA + DHA). The iFATS score provides a quantitative, individualized measure of how much a given dog has shifted away from a pro-inflammatory fatty acid environment toward an anti-inflammatory one, a direct biological readout of supplementation response.
Key findings: Daily EPA/DHA supplementation produced statistically significant shifts in red blood cell membrane fatty acid composition (increased EPA and DHA, decreased arachidonic acid) that correlated with clinical improvement in osteoarthritis signs. Dogs in the supplemented group showed measurable improvements over placebo. Fish oil was generally well tolerated.
Authors’ conclusion: Daily supplementation of a dog’s diet with EPA and DHA shifts blood fatty acid concentrations in a manner that correlates with relief of clinical signs of osteoarthritis. This is among the few canine nutraceutical interventions to demonstrate biomarker-confirmed clinical benefit in a properly powered randomized controlled trial.
Clinical implication: The Mehler study reframes how veterinarians should think about EPA and DHA supplementation in dogs. The benefit is not assumed, it is measurable, both clinically (owner-reported quality of life, lameness, mobility) and biochemically (iFATS, Omega-3 Index). For dogs that fail to respond clinically, biomarker testing can determine whether the issue is dose, formulation quality, individual absorption, or non-response.
6. Multi-Organ System Benefits
Heart, Brain, Skin, Kidneys & Eyes
While joint comfort is the most evidence-supported indication, the clinical relevance of EPA and DHA extends across virtually every organ system that depends on healthy inflammatory signaling, membrane integrity, or vascular function. Put simply, my clinical recommendation is that EPA/DHA be considered foundational nutritional support across the canine lifespan, with the joint-comfort benefit being one of several converging clinical justifications.
System-by-System Clinical Relevance
| Organ System | Role of EPA & DHA |
|---|---|
| Cartilage & Joints (primary indication) | Reduced cartilage matrix degradation, reduced synovial inflammation, reduced peripheral nociceptive sensitization, improved owner-reported quality of life. Most robust evidence base. See Sections 4 and 5. |
| Cardiovascular | EPA and DHA support healthy myocardial membrane composition, normal heart rhythm, and vascular endothelial function. This is particularly relevant in breeds predisposed to dilated cardiomyopathy and in dogs with chronic valvular disease as part of integrated cardiac care alongside veterinary cardiology management. |
| Brain & Cognitive Function | DHA is a primary structural component of neuronal membranes. It supports neurological development in puppies (working with breeders and developmental veterinarians for early-life nutrition), and contributes to cognitive function in senior dogs alongside other interventions for canine cognitive dysfunction (CCD). To that end, DHA supplementation is part of evidence-based geriatric canine wellness. |
| Skin & Coat | EPA reduces inflammatory dermatologic signaling, relevant for atopic dermatitis, allergic skin disease, and chronic pruritus. Meanwhile, DHA contributes to skin barrier lipid composition. Coat softness, reduced shedding, and reduced flaking are commonly reported owner-observed effects within 4–8 weeks of consistent supplementation. |
| Renal Function | EPA and DHA reduce glomerular inflammatory signaling and may slow progression of chronic kidney disease (CKD) in dogs as part of an integrated CKD management plan. For this reason, many veterinary CKD diets are formulated with elevated omega-3 content. |
| Ocular Health | DHA is concentrated in retinal photoreceptor outer segments and is essential to retinal function. Omega-3 supplementation is part of supportive care in some inflammatory ocular conditions including keratoconjunctivitis sicca (dry eye), where it has been studied as adjuvant therapy. |
| Immune & Inflammatory Balance | Production of resolvins, protectins, and maresins supports active resolution of inflammation across tissues. This is particularly relevant in chronic low-grade inflammatory states including obesity, allergy, and post-surgical recovery. |
| Senior Dog Wellness (synthesizing all of the above) | Senior dogs typically present with the full spectrum of age-related multi-system involvement: joint comfort, cognitive change, cardiac murmur, declining coat condition, and emerging renal compromise. EPA/DHA supplementation addresses multiple of these systems simultaneously through a single, well-tolerated intervention. Above all, foundational in my senior wellness protocols. |
7. Individual Variability
Why Two Dogs on the Same Dose Get Different Results
One of the most clinically important, and least appreciated, aspects of canine omega-3 supplementation is the substantial inter-individual variability in absorption, incorporation, and response. Specifically, two dogs of identical body weight, on identical doses of identical product, can end up with markedly different membrane EPA and DHA concentrations and correspondingly different clinical responses.
That said, this is not failure of the supplement; it is the biology of fatty acid metabolism. The variables driving inter-individual variability include:
Variables Affecting Omega-3 Response
Variable |
How It Affects Omega-3 Response in Dogs |
|---|---|
| Form of EPA/DHA in product | Natural triglyceride form is absorbed approximately 50% more efficiently than ethyl ester form on average, but with significant individual variation. Re-esterified triglyceride form falls between. This is the single largest product-level variable. |
| Co-administration with dietary fat | Omega-3 absorption is fat-dependent. A capsule given on an empty stomach absorbs poorly; on the other hand, the same capsule given with a meal containing dietary fat absorbs substantially better. Dose splitting with meals is clinically meaningful. |
| Baseline fatty acid status | A dog with severely depleted membrane EPA and DHA at baseline takes longer to reach therapeutic concentrations than a dog whose diet already includes some marine omega-3. The starting point matters. |
| GI absorption efficiency | Dogs with chronic GI conditions (IBD, EPI, post-surgical resections) have reduced fatty acid absorption. Consequently, dosing may need to be adjusted upward or split more aggressively. |
| Concurrent dietary omega-6 load | A dog on a high omega-6 diet (corn-fed protein, sunflower oil, refined grain-based foods) has competing substrate at the membrane and enzymatic level. Therefore, dietary omega-6 reduction amplifies omega-3 supplementation effect. |
| Body composition | Obese dogs sequester more fatty acids in adipose tissue, reducing the proportion reaching membrane phospholipids. As a result, lean body mass-based dosing is a more accurate framework than total body weight, particularly in overweight dogs. |
| Genetic / metabolic individuality | Dogs differ in the activity of desaturase and elongase enzymes that interconvert fatty acid species, in their basal inflammatory tone, and in their endogenous SPM production. These differences explain much of the residual variation in clinical response after all the above are controlled for. |
The clinical implication is that a single fixed dose for all dogs of a given body weight is necessarily a starting point, not an endpoint. Dogs that fail to respond to a standard dose may be inadequately dosed, may be receiving an inferior product form, may have absorption limitations, or may be among the genuine subset of low responders. In other words, without measurement, you cannot tell which.
8. The Omega-3 Index and iFATS
Personalizing Omega-3 Fatty Acids for Dogs
This is where the most practically important advance in canine omega-3 medicine sits. In particular, two complementary biomarkers can now be measured to verify and individualize EPA/DHA therapy: the Omega-3 Index and the iFATS (Inflammatory Fatty Acid Test Score). Both are derived from a small blood sample (often a dried blood spot), making them practical in real-world veterinary practice.
How the Two Biomarkers Compare
Biomarker |
What It Measures & How To Use It Clinically |
|---|---|
| Omega-3 Index | The percentage of EPA + DHA in red blood cell membrane fatty acids, expressed as a percentage of total fatty acids. Validated in dogs and cats. Reflects integrated EPA/DHA exposure over the prior several weeks, a stable, long-term marker of fatty acid status. Higher values indicate better omega-3 status. |
| iFATS (Inflammatory Fatty Acid Test Score) | The ratio of arachidonic acid to (EPA + DHA) in red blood cell membrane fatty acids, the algorithm featured in the Mehler et al. (2016) RCT. iFATS quantifies the balance between pro-inflammatory and anti-inflammatory substrate at the cell membrane level. Lower iFATS values indicate a less pro-inflammatory fatty acid environment. Notably, iFATS shifted favorably in the supplemented group of the Mehler study and correlated with clinical improvement. |
| How they fit together | Omega-3 Index tells you whether the dog is getting enough EPA and DHA. Meanwhile, iFATS tells you whether the resulting cell-membrane balance is meaningfully anti-inflammatory. Both should improve together with effective supplementation. If a dog’s clinical response is inadequate and either biomarker has not shifted appropriately, the dose, the product, or the absorption is the problem, not the omega-3 strategy. |
| Recommended use in practice | Baseline Omega-3 Index and/or iFATS prior to initiating supplementation. Recheck at 8–12 weeks. Use the result to adjust dose for non-responders and to confirm therapeutic response in clinically improved dogs. This is particularly valuable in working and performance dogs, in canine athletes, and in dogs being managed multimodally for osteoarthritis where the goal is reducing concurrent NSAID burden. |
“We have moved past the era of recommending fish oil and hoping it works. With the Omega-3 Index and iFATS, we can verify that the supplement is reaching the cell membrane, that the inflammatory fatty acid balance has shifted, and that the biological foundation for clinical benefit is actually in place. This transforms canine omega-3 therapy from an empirical recommendation into an individualized, measurable practice.”
— Dr. James S. Gaynor, DACVAA — Board-Certified Veterinary Specialist in Anesthesia & Pain Management
9. Omega-3 Dosage for Dogs: EPA + DHA Targets by Body Weight & Indication
Omega-3 dosage for dogs should be expressed in milligrams of combined EPA + DHA per day, not in milligrams of fish oil, not in capsule count, and not in teaspoons of unspecified oil. The clinical evidence base, including the Mehler et al. (2016) RCT, supports the following framework as a clinical starting point. Individual dosing should be refined using clinical response and, where available, Omega-3 Index and iFATS testing.
Dose Targets by Body Weight Category
Body Weight |
Daily EPA + DHA Target (Combined) |
|---|---|
| Small dogs (5–20 lbs) | Approximately 200–500 mg combined EPA + DHA daily, divided with meals. Lower end for general wellness and skin/coat support; higher end for joint-comfort indications. |
| Medium dogs (20–50 lbs) | Approximately 500–1,200 mg combined EPA + DHA daily, divided with meals. Increase to the higher end of the range for confirmed osteoarthritis, allergic dermatitis, or cardiovascular indication. |
| Large dogs (50–90 lbs) | Approximately 1,200–2,200 mg combined EPA + DHA daily, divided with meals. The Mehler et al. (2016) RCT used a clinically meaningful EPA + DHA dose in this range and produced both biomarker and clinical response in dogs with osteoarthritis. |
| Giant dogs (>90 lbs) | Approximately 2,200–3,500 mg combined EPA + DHA daily, divided with meals. Veterinary supervision recommended; biomarker-guided titration particularly valuable in this category. |
Per-Kilogram Dosing for Joint-Comfort Indications
Some dosing frameworks express omega-3 targets in milligrams per kilogram of body weight rather than by weight class. Two per-kg targets appear in the canine clinical literature, and they refer to different things, both can be useful depending on the clinical question:
EPA-specific target: For optimal joint health, dogs may receive approximately 50–60 mg/kg of EPA orally daily. This isolates the EPA component, which is the primary anti-inflammatory omega-3 driving the joint-comfort effect.
Combined EPA + DHA target: Published canine clinical literature has used doses on the order of 70 mg/kg/day of combined EPA + DHA, with measurable clinical benefit reported in dogs with osteoarthritis at this magnitude.
Why both matter: The EPA-only and EPA + DHA targets describe the same therapeutic window from two angles. Similarly, quality marine fish oils typically deliver EPA and DHA in roughly comparable amounts, so a product dosed to hit 70 mg/kg/day combined will generally also deliver EPA in the 50–60 mg/kg range. The per-kg framework is particularly useful in giant breeds and lean working dogs where total-body-weight categories may under- or over-dose.
Practical Administration Considerations
✔ Always with food: EPA/DHA absorption is fat-dependent. Administer with meals; bioavailability is meaningfully reduced when given on an empty stomach.
✔ Once daily or split twice daily: Once-daily and twice-daily dosing reach similar steady-state membrane concentrations, but split dosing produces more stable plasma profiles and is well-tolerated.
✔ Allow 8–12 weeks for full effect: Cell membrane fatty acid composition turns over gradually. Owners should be counseled to expect onset over weeks, not days. Reassess at 8 and 12 weeks.
✔ Monitor for GI signs: Loose stool or mild GI upset is the most common side effect, usually self-limiting. Reduce dose temporarily and titrate up.
✔ Bleeding-time considerations: At very high doses, omega-3s can mildly prolong bleeding time. In dogs scheduled for elective surgery, discuss timing with the surgical team. At standard doses this is generally not clinically significant.
10. Quality Matters: Triglyceride Form, Oxidation & Third-Party Testing
The omega-3 supplement category is among the most variable in pet nutraceuticals, both in EPA/DHA content versus label claim and in product oxidation status. Notably, two dogs given identical labeled doses of two different fish oil products can end up with materially different outcomes. Veterinarians should counsel owners on the following quality-defining variables:
Quality
Variable |
Why It Matters |
|---|---|
| Form: Natural triglyceride vs. ethyl ester | Natural triglyceride form (or re-esterified triglyceride) is absorbed substantially more efficiently than ethyl ester form. Many inexpensive fish oils are ethyl ester. In contrast, premium veterinary products including Peak Therapeutics Canine Omega Benefits use natural triglyceride form for maximal absorption. |
| Oxidation status | Omega-3 fatty acids oxidize on exposure to heat, light, and oxygen. Oxidized fish oil is at best ineffective and at worst pro-inflammatory, the opposite of the intended clinical effect. Therefore, products should be third-party tested for peroxide value, anisidine value, and TOTOX. Dark bottles, refrigeration after opening, and recent manufacture date all matter. |
| Heavy metals & contaminants | Marine fish oils carry the same heavy metal and persistent organic pollutant concerns as their source fish. Quality manufacturers use molecular distillation and certify low mercury, cadmium, lead, dioxin, and PCB content. Independent testing certificates should be available. |
| Source fish | Sustainably sourced, smaller, shorter-lived fish (anchovy, sardine, pollock, krill) generally accumulate fewer contaminants than large predatory species. Disclosure of source species is a quality marker. |
| EPA + DHA per serving (not total fish oil) | Read the label for combined EPA + DHA per serving. “1,000 mg of fish oil” is uninformative; “500 mg combined EPA + DHA” is what determines clinical dose. |
11. Integrating Omega-3 Fatty Acids for Dogs into a Multimodal Joint Wellness Protocol
As with cannabinoid therapy and other evidence-based nutraceuticals, the most clinically productive framework for canine omega-3 supplementation is as one component of a multimodal protocol, particularly for canine osteoarthritis, where multiple converging mechanisms produce outcomes that exceed any single intervention.
Components of an Effective Multimodal Protocol
Protocol Component |
Role in Multimodal Joint Wellness |
|---|---|
| EPA + DHA (Omega-3) | Foundational. Addresses cartilage matrix preservation, synovial inflammation, peripheral nociception, and active inflammatory resolution. Biomarker-verifiable. Receptor- and substrate-level mechanism. |
| Structural joint support | Glucosamine, chondroitin, hyaluronic acid, eggshell membrane, undenatured type II collagen, addresses the cartilage matrix and synovial fluid at the structural level. Different mechanism, complementary effect. |
| CBD / full-spectrum hemp | Engages the endocannabinoid system at the receptor level, modulating nociceptive signaling, inflammatory cytokine release, and anxiety associated with chronic discomfort. See Peak Therapeutics CBD for dogs resources. |
| NSAIDs (where indicated) | Veterinarian-prescribed NSAIDs remain a cornerstone of canine OA management. A consistent finding in clinical practice is that effective omega-3 and multimodal nutraceutical support reduces the dose or frequency of NSAID required, clinically meaningful for cumulative GI, hepatic, and renal exposure over the course of a chronic-care management plan. |
| Targeted exercise & rehabilitation | Controlled, low-impact exercise; underwater treadmill where available; range-of-motion work, maintains joint health, muscle mass, and proprioception. Pharmacologic comfort enables exercise; in turn, exercise sustains long-term joint function. |
| Weight optimization | Every pound of excess weight increases joint loading and adipose-driven inflammatory signaling. Weight optimization is among the highest-impact interventions in canine osteoarthritis management. |
| Regenerative medicine (where indicated) | Stem cell therapy, PRP, and intra-articular hyaluronate are emerging structural-level interventions for selected cases. Complementary to nutraceutical and pharmacologic support. |
12. Peak Therapeutics Canine Omega Benefits: Formulation & Quality Standards
Peak Therapeutics Canine Omega Benefits is the omega-3 fatty acid component of our integrated canine wellness line. Specifically, it is formulated to the same evidence standards applied across all Peak Therapeutics products: clinically meaningful EPA + DHA per serving, natural triglyceride form for maximal absorption, third-party tested for purity and oxidation, and aligned with the dosing framework supported by the published clinical literature, including the Mehler et al. (2016) RCT.
Product |
Formulation & Clinical Use |
|---|---|
| Canine Omega Benefits — Hypoallergenic | Hypoallergenic formulation for dogs with dietary sensitivities or food-allergic dermatologic disease. High concentration of combined EPA + DHA per serving. Natural triglyceride form. Independently third-party tested. Suitable as foundational daily supplementation across the canine lifespan. |
| Canine Omega Benefits — Beef Flavor | Beef-flavored formulation for owner-administration palatability. Same clinically meaningful EPA + DHA concentration and natural triglyceride form. Many owners find this format easiest for daily compliance, particularly in dogs that resist liquid supplementation directly. |
Quality Standards Across All Canine Omega Benefits Formulations
Veterinarian-Formulated: Developed in alignment with the published canine omega-3 clinical literature, with EPA + DHA concentrations targeted to support the daily dose ranges established in randomized controlled trials including Mehler et al. (2016).
Natural Triglyceride Form: Maximal bioavailability, the natural form in which EPA and DHA exist in fish, absorbed substantially more efficiently than ethyl ester preparations.
Third-Party Lab Tested: Every batch independently analyzed for EPA + DHA potency, peroxide and anisidine value (oxidation), heavy metals, and persistent organic pollutants.
Sustainably Sourced: Marine sourcing aligned with sustainable fishery standards, prioritizing smaller, shorter-lived species with lower contaminant profiles.
Clinically Meaningful Concentration: EPA + DHA per serving is matched to the dose ranges supported by canine clinical evidence, not the under-dosed levels that are common in lower-cost fish oils marketed for pets.
Explore Peak Therapeutics Canine Omega Benefits
Hypoallergenic Formula Beef Flavor Formula
Veterinarian-formulated. Natural triglyceride form. Third-party lab tested.
13. Frequently Asked Questions — Omega-3 Fatty Acids for Dogs
Are Omega-3 fatty acids safe for dogs?
Yes. At therapeutic doses, EPA and DHA from quality marine sources have a well-established safety profile in dogs. The most common side effect is mild GI upset (loose stool), usually self-limiting and dose-responsive. At very high doses, mild prolongation of bleeding time has been reported, which is rarely clinically significant but should be considered around elective surgery. Importantly, quality and oxidation status of the product matter for safety as much as dose; oxidized fish oil is the more meaningful real-world safety concern.
What is the best Omega-3 dosage for dogs?
Dose by combined EPA + DHA per day, not by total fish oil milligrams. As a clinical starting framework: 200–500 mg/day for small dogs (5–20 lbs), 500–1,200 mg/day for medium dogs (20–50 lbs), 1,200–2,200 mg/day for large dogs (50–90 lbs), and 2,200–3,500 mg/day for giant dogs. Higher end of each range for confirmed osteoarthritis, allergic dermatitis, or cardiovascular indications. Refine with clinical response and Omega-3 Index/iFATS testing where available.
How long do Omega-3 fatty acids take to work in dogs?
Cell membrane fatty acid composition turns over over weeks. Skin and coat improvements are commonly reported by owners within 4–8 weeks. Joint comfort improvements typically become apparent at 8–12 weeks of consistent daily supplementation, which mirrors the timeline reported in randomized controlled trials including Mehler et al. (2016). Dogs that show no benefit at 12 weeks should have dose, product form, and ideally Omega-3 Index/iFATS reassessed.
What is iFATS and why does it matter for Omega-3 fatty acids in dogs?
iFATS (Inflammatory Fatty Acid Test Score) is the ratio of arachidonic acid to (EPA + DHA) in red blood cell membrane fatty acids. It quantifies how pro-inflammatory or anti-inflammatory the dog’s cellular fatty acid environment is. iFATS shifts favorably with effective EPA/DHA supplementation, and these shifts correlated with clinical improvement in osteoarthritic dogs in the Mehler et al. (2016) randomized controlled trial. iFATS, alongside the Omega-3 Index, is the most useful biomarker tool for individualizing Omega-3 fatty acids for dogs.
Why do some dogs respond to Omega-3 fatty acids and others don’t?
Inter-individual variability is real and clinically important. Variables include the form of EPA/DHA in the product (natural triglyceride vs. ethyl ester), co-administration with dietary fat, baseline fatty acid status, GI absorption efficiency, concurrent dietary omega-6 load, body composition, and genetic differences in fatty acid metabolism. A dog that fails to respond clinically may be inadequately dosed, may have absorption limitations, or may be a low responder; biomarker testing (Omega-3 Index, iFATS) distinguishes these scenarios.
Is fish oil better than flaxseed oil for dogs?
For clinical dosing, yes. Flaxseed oil supplies ALA (alpha-linolenic acid), which dogs convert to EPA and DHA at very low efficiency, single-digit conversion rates. In contrast, marine fish oil supplies preformed EPA and DHA directly. For meaningful joint, cardiovascular, neurological, or dermatologic benefit, marine sources are required. Plant omega-3 sources alone do not reach the membrane EPA/DHA levels associated with the clinical benefits established in the canine literature.
Can dogs take Omega-3 fatty acids alongside NSAIDs?
Yes. Omega-3 fatty acids for dogs are commonly used alongside veterinarian-prescribed NSAIDs for osteoarthritis, with the clinical goal of reducing the cumulative NSAID dose required for adequate comfort. The mechanisms are complementary rather than redundant: NSAIDs block COX enzymes acutely, while EPA/DHA shift the underlying substrate pool and produce specialized pro-resolving mediators. Discuss any concurrent supplement regimen with the prescribing veterinarian.
Which Omega-3 product is best for senior dogs?
Senior dogs benefit most from foundational daily EPA + DHA supplementation at the higher end of their body-weight dose range, given the multi-system relevance: joint comfort, cognitive function, cardiovascular and renal support, and skin/coat condition. Peak Therapeutics Canine Omega Benefits in either the Hypoallergenic or Beef Flavor formulation is clinically appropriate. Combine with structural joint support and CBD-based ECS support for comprehensive senior multimodal wellness.
How are Omega-3 fatty acids for dogs different from CBD for dogs?
Different mechanism, complementary clinical effect. CBD for dogs engages the endocannabinoid system at the receptor level, modulating nociceptive signaling, inflammatory cytokine release, and stress responses. Meanwhile, omega-3 fatty acids for dogs shift the fatty acid substrate pool feeding inflammatory enzyme systems, producing fewer pro-inflammatory eicosanoids and more specialized pro-resolving mediators. Used together, they address chronic inflammation and discomfort through independent pathways, which is why both are foundational components of my multimodal canine wellness protocols.
Should I get my dog’s Omega-3 Index tested?
For most dogs on consistent daily supplementation with a quality product who are clinically responding, formal biomarker testing is not required. However, in dogs that fail to respond clinically, in working or performance dogs where measurable optimization is valuable, in dogs with confirmed osteoarthritis being managed multimodally to reduce NSAID burden, or in dogs with complex dermatologic or cardiovascular indications, Omega-3 Index and iFATS testing provide objective, individualized information that materially changes dosing decisions. Discuss with your veterinarian.
14. References
Mehler SJ, May LR, King C, Harris WS, Shah Z. A prospective, randomized, double-blind, placebo-controlled evaluation of the effects of eicosapentaenoic acid and docosahexaenoic acid on the clinical signs and erythrocyte membrane polyunsaturated fatty acid concentrations in dogs with osteoarthritis. Prostaglandins, Leukotrienes and Essential Fatty Acids. 2016;109:1–7. doi:10.1016/j.plefa.2016.03.015
Harris WS, Jackson KH, Carlson H, Hoem N, Dominguez TE, Burri L. Derivation of the Omega-3 Index from EPA and DHA Analysis of Dried Blood Spots from Dogs and Cats. Veterinary Sciences. 2022;10(1):13. doi:10.3390/vetsci10010013
Roush JK, Cross AR, Renberg WC, et al. Evaluation of the effects of dietary supplementation with fish oil omega-3 fatty acids on weight bearing in dogs with osteoarthritis. Journal of the American Veterinary Medical Association. 2010;236(1):67–73.
Roush JK, Dodd CE, Fritsch DA, et al. Multicenter veterinary practice assessment of the effects of omega-3 fatty acids on osteoarthritis in dogs. Journal of the American Veterinary Medical Association. 2010;236(1):59–66.
Fritsch DA, Allen TA, Dodd CE, et al. A multicenter study of the effect of dietary supplementation with fish oil omega-3 fatty acids on carprofen dosage in dogs with osteoarthritis. Journal of the American Veterinary Medical Association. 2010;236(5):535–539.
Bauer JE. Therapeutic use of fish oils in companion animals. Journal of the American Veterinary Medical Association. 2011;239(11):1441–1451.
Lenox CE, Bauer JE. Potential adverse effects of omega-3 fatty acids in dogs and cats. Journal of Veterinary Internal Medicine. 2013;27(2):217–226.
Gaynor JS, Muir WW (eds). Handbook of Veterinary Pain Management, 3rd Edition. Mosby/Elsevier, 2015.
15. About Dr. James S. Gaynor, DVM, MS, DACVAA

Education
- BA, Biology — The Colorado College, Colorado Springs, CO, 1983
- DVM — The Ohio State University, Columbus, OH, 1988
- Anesthesiology Residency & MS (Cardiac Physiology) — The Ohio State University, Columbus, OH, 1992
Board Certifications & Credentials
- Diplomate, American College of Veterinary Anesthesiologists (DACVAA), 1993
- Board Certified, Academy of Integrative Pain Management, 2004
- Certified, International Veterinary Acupuncture Society, 1999
- Certified Veterinary Pain Practitioner, International Veterinary Academy of Pain Management, 2011
- Certified CBD Consultant, Cannabinoid Medicine Studies, 2020
Academic & Clinical Career
- Assistant/Associate Professor & Section Head of Anesthesiology, Colorado State University College of Veterinary Medicine, 1992–2003
- Medical Director & Staff Anesthesiologist, Peak Performance Veterinary Group, Frisco, CO, 2004–2021
- Medical Director & Staff Anesthesiologist, Colorado Animal Specialty and Emergency, Boulder, CO, 2021–2026
- Staff Anesthesiologist, Buffalo Mountain Animal Hospital, Dillon, CO, 2026–present
- Medical Director & Staff Anesthesiologist, Black Dog Veterinary Anesthesia Services, Breckenridge, CO, 2026–present
- Associate Editor, Frontiers in Veterinary Sciences, 2025–present
Published Books
- Cannabis Therapy in Veterinary Medicine: A Complete Guide — Co-editor & Author (Springer, 2021).
- Handbook of Veterinary Pain Management, 3rd Edition — Lead Editor & Author (Mosby/Elsevier, 2015).
© 2026 Peak Therapeutics | Authored by Dr. James S. Gaynor, DVM, MS, DACVAA | peaktherapeutics.net
This article is for educational and informational purposes only and does not constitute veterinary medical advice. Consult a licensed veterinarian before initiating any nutraceutical protocol for your dog. These statements have not been evaluated by the Food and Drug Administration. This product is not intended to diagnose, treat, cure, or prevent any disease.
Recent Comments